How to conduct a root cause investigation using DMAIC principle
- Kazi
- Last modified: March 15, 2025
In GMP facilities, root cause investigation is carried out in order to control quality concern issues methodically. Such exercise includes major deviation investigations, complaint investigations, incidents, repeat incidents, defects, QC out of specification results investigation, etc. Identification of root cause is the final step of an investigation followed by implementation of suitable, long-term preventative actions as a permanent fix.
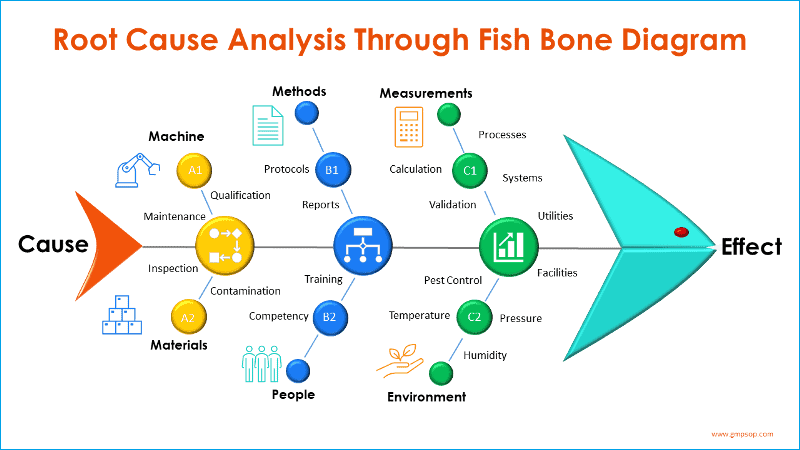
A very popular and widely used tool for root cause investigation is Fish Bone analysis.
It is also called a Cause-and-Effect diagram as the process starts from the mouth of the fish (which is the Effect), and the pursuit is to identify the exact root causes that have resulted in or contributed to the Effect.
The tool was named after its creator, Kaoru Ishikawa; hence, it is also known as Ishikawa diagrams.
Table of Contents
DMAIC root cause investigation tool
Another popular tool for root cause investigation is based on DMAIC (Define – Measure – Analyse – Implement – Control) principle which involves thorough inspection of wider aspects of the facility and processes.
Typically, a DMAIC Investigation tool is used if the root cause of a deviation is not known and there is a necessity to perform an in-depth investigation with an effort to identify root cause/s which are hidden beneath the process and not so apparent.
You should be careful that a DMAIC investigation exercise does not need to be carried out for every unplanned and minor deviation situation as this exercise involves wider resources to be deployed and contributions from cross functional teams.
As a rule of thumb you should initiate DMAIC root cause investigation if one or more of the following occur:
- You cannot be determine the cause of the unplanned deviation with certainty.
- There is a probable cause or set of causes based on available evidence but the causes are not confirmed as the root cause.
- A number of unplanned deviations that indicates repeated trends or when there are repeated trends indicated by other quality systems, such as complaints, periodic product quality review etc.
You should not use DMAIC root cause investigation as a substitution of usual unplanned deviation investigation. Rather, the tool will help you to undetkae extended investigation. The findings of the investigation are attached with corresponding deviation.
As the root cause is determined, corrective and preventative actions (CAPA) are implemented to stop recurrence of similar incidents or defects.
Scopes of DMAIC root cause investigation
Through DMAIC investigation process you can gather facts by interviewing colleagues, batch record review, complaint files, retain samples, procedures and instructions, quality control testing, in-process monitoring, stability data, trends in deviations, previous investigations, change control, product quality reviews, equipment and utility maintenance programs etc. as appropriate.
The investigation might be extended to other batches of the same product, other products, related processing areas and equipment that may be associated with the specific failure or incident as required. Sometime, facts need to be gathered from other manufacturing sites and relevant third party contractors, if required.
The five steps to DMAIC root cause investigation
The DMAIC root cause investigation process follows a sequential five steps question and answer pattern. It is important you complete each section with specific responses in order to reach to a plausible and true root cause. The DMAIC investigation process includes the following sections in chronological order.
Step 1: DEFINE (problem definition)
This is the first section of the root cause investigation. The section is designed with list of questions to participants in order to define the problem, its history and to outline any work that has been done so far. Typical questions during the defining stage are:
- What is the problem / incident? (record exactly what actually happened)
- When did it happen? (record the date and time of incident)
- Where did it happened? (to record specifically what process, equipment or facilities were impacted)
- Who was working when the incident was discovered? (record who had found the incident first time)
- What actions are taken immediately to fix the problem? (to record briefly the actions taken and by whom?)
- How long did it take to fix the problems? (to determine incident lost time)
- Has this happened before? (to identify history or trend on similar incident)
- What actions were taken before? (to record any changes made previously)
250 SOPs, 197 GMP Manuals, 64 Templates, 30 Training modules, 167 Forms. Additional documents are included each month. All written and updated by GMP experts. Check out sample previews. Access to exclusive content for an affordable fee.

250 SOPs, 197 GMP Manuals, 64 Templates, 30 Training modules, 167 Forms. Additional documents are included each month. All written and updated by GMP experts. Check out sample previews. Access to exclusive content for an affordable fee.
Step 2: MEASURE (understanding the process)
At this step, your subject matter experts draw a detailed process map on a piece of paper to help them understand the sequential activities involved in the process by which the incident was discovered.
As the outline of the process map is completed, the participants attempt to mark possible area/s of weakness where the deviation/incident has occurred.
A simple process mapping example for incoming goods release may involve sequentially:
- Receipt of new batch of raw materials
- Reconciliation between requisition and picking slip
- Decision - If both do not match, reject the material; or
- If matches, store the material in quarantine cage
- Samples taken for QC testing
- Decision - testing does not pass – reject the lot; or
- Testing conforms specifications
- QA review the Certificate of Analysis (C of A)
- Decision - C of A does not meet internal specification - reject the lot; or
- C of A meet internal specifications - approve the lot
- Release for further processing, etc.
During the measurement step participants try to mark possible areas of concerns on the process map which may be responsible for repeat incidents and worth to analyse more in depth.
Step 3a: ANALYSIS (process analysis)
This section is designed to list if there were significant changes to process which might have contributed to repetitive incidents. The participants also need to identify and list the process controls and possible non value adding steps.
Step 3b: ANALYSIS (cause and effect analysis; Fishbone diagram)
This section is designed to perform a cause and effect analysis using a fishbone diagram (also known as Ishikawa diagrams). During this process you should add the effect (Problem) at the front of the fish head and progressively create branches of possible causes from the six process areas and systems.
Participants will brain storm on each of six broad categories or systems which are:
- Machine
- Methods
- Measurements
- Materials
- People, and
- Environments
250 SOPs, 197 GMP Manuals, 64 Templates, 30 Training modules, 167 Forms. Additional documents are included each month. All written and updated by GMP experts. Check out sample previews. Access to exclusive content for an affordable fee.
A fishbone diagram is a visual tool and the exercise is particularly helpful for you to categorise possible causes of the problem which might otherwise be not too obvious, as the common human tendency is to land into a conclusion too early based on someone’s perception of what might have happened as opposed to what actually happened.
Step 3c: ANALYSIS (5 WHYs, Pareto Chart)
In this section you will mark the possible causes of the problem marked on the Fishbone diagram. Each of the potential causes is than spread down by asking the question “WHY” up to five successive occasions or up to the point the participants feel the best possible root cause is already attained.
Your team should brainstorm all the possible causes of the problem. Ask “Why does this happen?” As each idea is given, a branch (bone) is drawn from the appropriate category.
Causes can be written in several places if they relate to several categories. Again ask “Why does this happen?” about each cause. Write sub-causes by branching off the cause branches.
Continues to ask “Why?” and generate deeper levels of causes and continue organizing them under related causes or categories. This will help you to identify and then address root causes to prevent future problems.
If found beneficial perform a Pareto analysis separately to show the fewest (20%) most significant causes which have been causing the highest (80%) level of effects.
Step 4: IMPROVE (Evaluate solutions)
As you have identified possible solutions in the analysis step 3c, each of the solution is then placed within a matrix which is best suited based on their weights measured with the degree of benefit and degree of difficulty during the implementation stage.
The solutions are grouped into four possible placements within the matrix which are:
i. Stars (High benefit, Low difficulty)
These solutions should be implemented with reasonable efforts which can contribute highly to stop recurrence of the incident.
ii. Quick Wins (Low benefit, Low difficulty)
These solutions should be implemented readily which may contribute to stop recurring incident.
iii. Extra Effort needed (High benefit, High difficulty)
These solutions are relatively hard and lengthy to implement. However, once implemented, these can effectively prevent such incidents.
iv. Forget It (Low benefit, High difficulty)
These solutions are perceivably the least effective but harder to implement. These possible solutions can be discarded.
Step 5: CONTROL (Implement solutions)
This final step involves listing the most effective and reasonable action controls to be implemented with a view to improve the problem areas.
If a system or process change is necessary, you should raise a change request and assess the potential impacts of those changes on the system or process. Streamline all documentation to reflect the change as a permanent basis.
Conclusion
In conclusion, the root cause investigation can be most effective when performed systematically, as described in the DMAIC five-step principle and fishbone diagram.
Some tips can be followed while brainstorming to maximize the participation of the participants in the pursuit of finding the root cause.
i. Use team approach. Establish a small group of people with the knowledge, time, authority and skill to solve the problem and implement corrective actions. The group must select a team leader.
ii. Describe the problem in measurable terms. Specify the internal or external customer problem by describing it in specific terms.
iii. Implement and verify short-term corrective actions. Define and implement those intermediate actions that will protect the customer from the problem until permanent corrective action is implemented. Verify with data the effectiveness of these actions.
iv. Define and verify root causes. Identify all potential causes that could explain why the problem occurred. Test each potential cause against the problem description and data. Identify alternative corrective actions to eliminate root cause.
v. Verify corrective actions. Confirm that the selected corrective actions will resolve the problem for the customer and will not cause undesirable side effects. Define other actions, if necessary, based on potential severity of problem.
vi. Implement permanent corrective actions. Define and implement the permanent corrective actions needed. Choose on-going controls to ensure the root cause is eliminated. Once in production, monitor the long-term effects and implement additional controls as necessary.
vii. Prevent recurrence. Modify specifications, update training, review work flow, improve practices and procedures to prevent recurrence of this and all similar problems.
viii. Congratulate your team. Recognize the collective efforts of your team. Publicize your achievement. Share your knowledge and learning.

Author: Kazi Hasan
Kazi is a seasoned pharmaceutical industry professional with over 20 years of experience specializing in production operations, quality management, and process validation.
Kazi has worked with several global pharmaceutical companies to streamline production processes, ensure product quality, and validate operations complying with international regulatory standards and best practices.
Kazi holds several pharmaceutical industry certifications including post-graduate degrees in Engineering Management and Business Administration.